Efficiency of remote blood pressure monitoring in outpatients with hypertension: a pilot project in a city ambulatory care clinic
Hypertension (HTN) is the main contributor (~42%) to cardiovascular disease pattern, being simultaneously not only one of the main risk factors for complications, but also significantly decreasing life expectancy due to premature disability [1]. Decrease in systolic blood pressure (SBP) by 10 mm Hg is associated with a significant reduction in risk of coronary artery disease by 20%, stroke by 17%, heart failure and all-cause death by 27% and 13%, respectively [2]. According to a metaanalysis by Thomopoulos C, et al. differences in SBP levels 12 mm Hg and diastolic blood pressure (DBP) 5 mm Hg are associated with significant reductions in all unfavorable outcomes, including mortality. Blood pressure (BP) decrease, regardless of antihypertensive drugs (AHD) taken, is associated with a decrease in the risk of stroke and most cardiovascular events [3].
Effectiveness of hypertension treatment depends not only on the correct and timely diagnosis and choice of the optimal treatment strategy, but also on patient medical adherence [4]. BP values obtained from blood pressure self-monitoring (BPSM) can be a valuable addition to office ones in the diagnosis of HTN and monitoring the treatment effectiveness. BP data recorded in by BPSM correlates more strongly with target organ damage and the prognosis of the disease than office blood pressure, and its predictive value is comparable to the data obtained with 24-hour monitoring, after adjusting for sex and age [5]. BPSM has been proven to increase patient medcial adherence [6]. According to the 2020 Russian Society of Cardiology guidelines, telemonitoring of systemic hemodynamic parameters with data transmission to a medical institution is recommended for patients with HTN (level of evidence, B; class of recommendations, I) [7]. In a pilot project based on ambulatory care clinic, the aim was to assess the effectiveness of remote blood pressure monitoring in achieving target values and increasing medical adherence of patients, as well as to assess ambulance call rate and changes in prescribing fixed-dose combinations.
Material and methods
For remote BP monitoring, including using automatic monitors with the function of data transmission, on the basis of Voronezh City Clinical Polyclinic № 1, 1,121 patients with HTN were included. The study was approved by the ethics committee of the N. N. Burdenko Voronezh State Medical University. There were following inclusion criteria: patients with hypertension over 18 years of age, signed informed consent, dispensary observation due to HTN, regular intake of antihypertensives, absence of severe comorbities (diabetes with a glycated hemoglobin level >9%, Child-Pugh score class B and C liver cirrhosis, chronic kidney disease with a glomerular filtration rate <30 ml/min/1,73 m2, severe asthma, active cancer, mental illness). All patients signed informed consent. The clinical characteristics of patients are presented in Table 1.
Table 1
Clinical and demographic characteristics of patients in the remote BP monitoring group

Abbreviations: CAD — coronary artery disease, GFR — glomerular filtration rate.
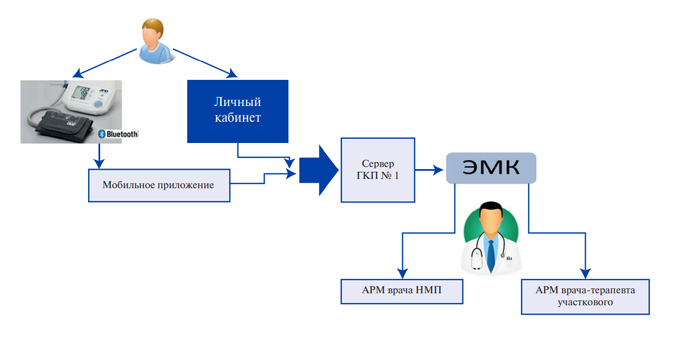
The patients were divided into 3 groups: patients who transmitted data from BP monitor using installed mobile application (group 1, n=35); those who independently measured BP and entered the values into personal account (group 2, n=200); those who kept a self-management paper diaries (group 3, n=886) (Figure 1).
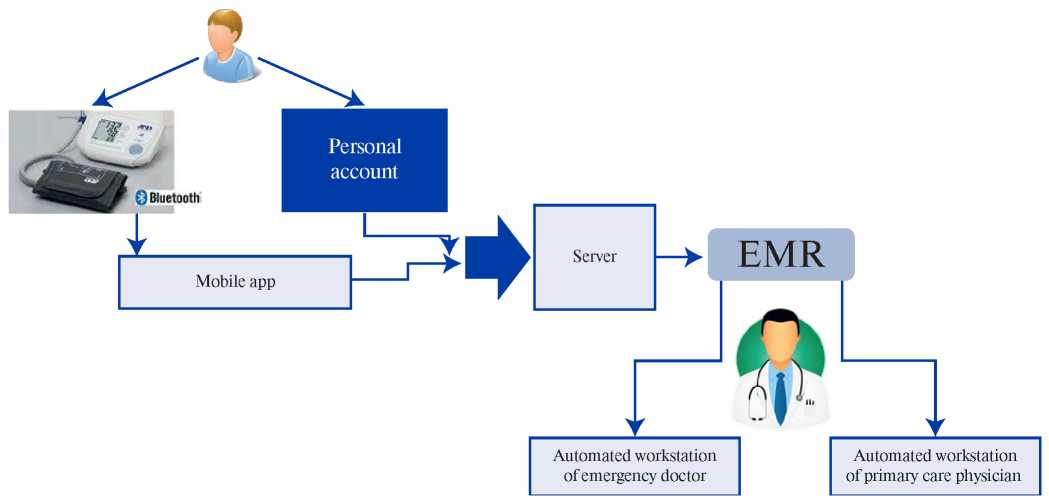
Figure 1. Model of remote BP data transmission.
Abbreviation: EMR — electronic medical record.
All patients were trained in the BPSM. It was recommended to independently measure blood pressure twice a day. Home SBP <135 mm Hg and DBP <85 mm Hg were considered as target.
Patients of group 1 received BP monitors A&D UA-911BT (Japan) with data transfer via Bluetooth. Each monitor had an internal number to identify the patient in the healthcare information system (HIS). Group 2 patients entered their blood pressure values into their personal records 2 times a day before they reached their target values, and once they reached their target values, they entered them once a day. The data entered by the patient in the selfmonitoring diary or transmitted from a smartphone were transferred to the HIS server of the medical organization and reflected in the patient’s personal electronic medical record. The attending physician and emergency room physician saw the results of the blood pressure measurement in the Tonometry module from the automated workstation. The HIS automatically calculated the average value of SBP and heart rate for a certain time interval. When SBP >150 mmHg was measured, a physician received an alert message, which ensured prompt decisionmaking on treatment adjustments by making an appointment with the attending physician. In the event of an increase in systolic blood pressure >170 mmHg, a telephone call was made in advance to decide whether or not an emergency treatment was required.
Group 3 patients were given a self-monitoring diary when they filled in their informed consent. Patients were advised to contact the attending physician by telephone if their blood pressure rose above the tolerance level (individual for each patient). The nurse made structured telephone contact at least once a week until the patients reached their target BP values, clarified their BP values and, if necessary, set a date and time for a visit to the doctor. The achievement of BP control was assessed using BPSM data, including at interim visits to the doctor’s office.
Treatment adherence was assessed using the Moriski-Green scale at face-to-face visits [8]. The Moriski-Green scale consists of four items relating to the patient’s attitude towards taking medication, completed by the patient. Alternatively, the physician can read out the questions and mark the answers. In the original scale, each item is scored on a “yes” or “no” basis, with a “yes” score of 0 and a “no” score of 1. Patients with a score of 4 are considered committed to treatment, <4 are not committed to treatment.
After 6 months of follow-up, the following measures were analyzed: the achievement of target SBP values (<135 mm Hg), adjustments in therapy and the number of drugs in the patient needed to achieve the target BP values, as well as adherence to treatment, changes in the number of emergency medical calls due to BP increase.
Results were analyzed using Statistica 10 package (Dell Software Company, USA). Descriptive statistics with calculation of mean values (M), standard deviation, and standard error (m) were used. The normality of distribution was analyzed using the graphical histogram, the Kolmogorov-Smirnov and Lilliefors tests, as well as determining asymmetry, kurtosis and their standard errors. Univariate and multivariate analysis of variance were used as methods of statistical analysis to identify differences between the mean values. The threshold level of statistical significance was 0,05.
Results
Thirteen (1,1%) patients (8 males and 5 females), 11 of whom were of working age, dropped out of the study within 6 months. Five patients dropped out for technical reasons (difficulty in entering data) during the first month and 5 patients dropped out due to employment after reaching the target BP values. Four patients were lost in contact (did not answer the phone).
According to the survey, only 15,2% (n=171) of patients had self-monitored blood pressure before the study. The initial target BP values (<140/<90 mmHg) were recorded in 14,5% (n=162) of the patients according to their outpatient medical records. During the 6 months of the study a significant decrease of BP was observed in the group of patients with remote BP monitoring in general, and the proportion of patients who reached the target values of BP increased by 3 times, which occurred against the background of the 1,7-fold increase in the frequency of dual AHT, 2-fold increase in triple therapy and 2,5fold increase in fixed-dose combinations (Table 2). Angiotensin-converting enzyme inhibitors were the most frequently prescribed AHD. At the same time, there was an increase in the prescription of calcium channel blockers by 13%, angiotensin II receptor antagonists by 12%, and diuretics by 11% (Figure 2). After 6 months, the Moriski-Green score increased from 2,15 to 3,18, and the proportion of patients committed to AHT was 3,1 times (Table 2). In general, remote BP monitoring promoted a more aggressive approach to prescribing combined AHT, but even with this strategy, only 43,1% of patients reached their target BP values.
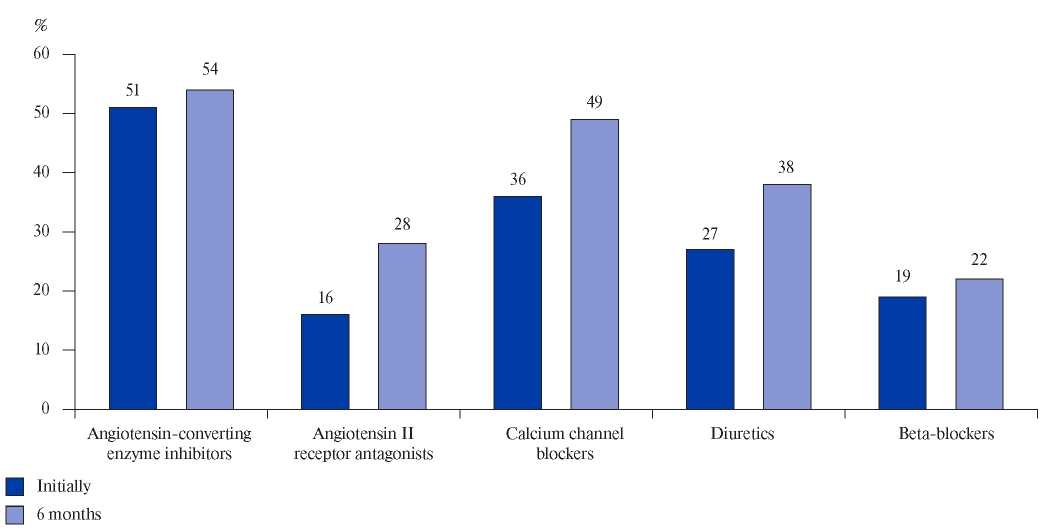
Figure 2. Dynamics of the appointment of antihypertensives’ groups.
Table 2
Dynamics of the parameters of the effectiveness of 6-month remote BP monitoring in the general group (n=1121)

Note: * — p<0,05, ** — p<0,01, the significance of differences between the baseline and achieved values.
Abbreviations: AHT — antihypertensive therapy, BP — blood pressure, DBP — diastolic blood pressure, SBP — systolic blood pressure.
The use of automatic BP monitors with remote data transmission in group 1 was associated with a 5,4-fold (up to 77,1%) increase in the proportion of patients achieving target BP values, a 2,4-fold (up to 60,0%) increase in the proportion receiving AHT in fixed-dose combinations and a 4,9-fold (up to 82,9%) increase in medical adherence (Table 3).
Table 3
Dynamics of the parameters of the effectiveness of 6-month remote BP monitoring in various groups

Note: * — p<0,01, the significance of differences between the baseline and achieved values.
Abbreviation: BP — blood pressure.
During the follow-up period, 11 patients (all of whom filled out paper-based self-monitoring diaries) had cardiovascular complications: 8 patients were diagnosed with non-fatal ischaemic stroke and 3 with non-fatal myocardial infarction. Of the 8 patients who had ischaemic stroke, 5 patients had irregular BP measurements and were taking combined AHT. Six patients had comorbid complications (diabetes, chronic kidney disease). Of the 11 patients, 7 continued to fill out self-monitoring diaries after the events and were seen by specialists, while 3 patients had pronounced cognitive impairment after the ischemic stroke.
During the 6 months of the study compared to the same period before the project, the number of emergency calls for due to BP increase decreased by 14,8% (Table 2).
Thus, the use of remote BP monitoring, including remote BP monitors, was associated with improved follow-up of patients with HTN over 6 months.
Discussion
The remote patient follow-up model is the most relevant and acceptable, aiming to analyze large numbers of patients at one time, using automatic or semi-automatic mechanisms to summarize information. Remote patient follow-up can theoretically help to reduce the number of visits associated with disease exacerbation as well as adverse life-threatening consequences [9]. Based on an economic analysis of remote BP monitoring in the Russian Federation, the project should be considered as not only efficient but also fast-paying, fully implementable by regional forces [10].
A meta-analysis of the efficacy of remote BP monitoring in patients with HTN summarized the results of 46 randomized controlled trials, which together included 13875 patients. The meta-analysis showed that, compared with conventional treatment, remote monitoring reduced clinical SBP and DBP by 3,99 mm Hg (p<0,001) and 1,99 mm Hg (p<0,001), respectively. The use of telemonitoring promoted BP normalization (relative risk, 1,16; p<0,001) [11]. However, a systematic review by Milevski M, et al. highlights a number of shortcomings in the use of remote BP monitoring. The authors note the small size of the evidence base for BP monitoring in patients with HTN. The results obtained using smartphone apps are also questioned. Errors made in the measurement of BP by patients, as well as reduced adherence due to the lack of staff attention to the results obtained, according to the authors, play against the use of telemedicine in BP monitoring [12].
The Saratov Research Institute of Cardiology developed remote BP monitoring technology based on mobile phone text messages in 2012, where the effectiveness of remote BP monitoring technology in HTN patients was evaluated on the basis of clinical guideline compliance indicators. The evaluation of remote BP monitoring in HTN patients made it possible to determine the improvement of the performance of the most significant therapeutic measures after its implementation [13]. Thus, all HTN patients (n=97) began to regularly report BP measurement results to their attending physician, and physicians, in turn, were more likely to prescribe combined AHT (increase from 70% to 82%, p<0,05) for uncontrolled BP, which was accompanied by a significant increase in the frequency of reaching the target BP. At the end of 12-month follow-up, mean SBP and DBP was 130,5±10,4 and 81,8±7,3 mm Hg (p<0,05). According to American research, bi-directional automated text messaging is an effective way to collect patient BP data. Text- message reminders alone are an effective way of encouraging patients to record BP measurements [14][15][16].
Significant reductions in SBP and DBP by an average of 15 mm Hg and 11 mm Hg (p<0,05) at six-month follow-up in this study demonstrates the effects of remote control and associated changes in AHT tactics — an increase in the proportion of patients prescribed dual AHT by 1,7 times, triple therapy by 2 times, and fixed-dose combinations by 2,5 times. In a study at the Saratov Research Institute of Cardiology, the proportion of patients using combined AHT increased by 17,1% after one year of follow-up, while the proportion of patients receiving combination therapy at baseline differed significantly (39,2% and 70%), which may have affected the achieved SBP and DBP values [13].
The results of this study indicate that the use of remote BP monitoring for 6 months is associated with a 3,1-fold increase in adherence to AHT. In addition, there was a 12,5% reduction in the ambulance call rate (Table 2).
The main problematic issues encountered in this pilot project are patients’ lack of adherence to lifestyle recommendations and insufficient adherence to treatment precisely after target BP levels have been achieved, especially among working patients. A special role in the functioning of the project is played by information technology (data exchange, telemedicine), training of medical staff and patients [17].
The issues of treatment adherence and patient motivation for lifestyle changes in the use of remote BP monitoring require further research.
A limitation of the study is its non-randomized, non-comparative design.
Conclusion
The use of remote BP monitoring methods, including BP monitors with automated data transmission, increases the prescription rate of combined antihypertensive therapy (dual AHT from 25,8 to 43,3%, triple therapy — from 11,5 to 22,9%, and fixed-dose combinations — from 25,4 to 51,6%) and proportion of patients who achieved the target BP (from 14,5 to 43,1%), as well as decreases the ambulance call rate from 19,3 to 16,9%.
Further 12-month implementation of the project will assess the cost-effectiveness of remote BP monitoring, including by reducing the ambulance call rate.

Чтобы читать статью войдите с логином и паролем от scardio.ru
Keywords
For citation
Sharapova Yu.A., Starodubtseva I.A., Villevalde S.V. Efficiency of remote blood pressure monitoring in outpatients with hypertension: a pilot project in a city ambulatory care clinic. Russian Journal of Cardiology. 2020;25:4149. https://doi.org/10.15829/1560-4071-2020-4149
Copy