Идеальный шторм: клинический случай множественной (мозговой, коронарной, почечной и селезеночной) эмболии у пациента с фибрилляцией предсердий
Аннотация
Неклапанная фибрилляция предсердий (ФП) является наиболее частой причиной артериальной тромбоэмболии, особенно при ишемическом инсульте. За исключением инсульта, ФП-ассоциированные эмболии обычно недооцениваются, однако являются не менее важными. В текущей работе описан редкий случай одновременной множественной эмболии у 70-летней женщины с постоянной формой ФП.
Introduction
Atrial fibrillation (AF) carries a significant health care burden. Other than stroke AF-associated embolic events are usually underestimated but may have at least similar clinical or prognostic importance. We present a rare case of acute multisite embolisms into coronary, brain, spleen and renal vessels in a patient with permanent AF.
History of presentation, past medical history
A 70-year-old woman with previous history of hypertension and AF (CHA2DS2-VASc score-3, HAS-BLED score-2) presented with acute chest pain, profuse sweating, and neurological symptoms such as dysarthria, dizziness and weakness (NIHSS-2). The symptoms appeared 4 hours before arrival. She was hypotensive (100/80 mm Hg) with heart rate 35 beats per minute, respiratory rate 22 breaths per minute and oxygen saturation 88% on room air. No cardiac murmurs were audible. Her baseline medications were acetylsalicylic acid, enalapril and bisoprolol.
Twelve-lead electrocardiography showed Frederick syndrome with T wave inversion in III and AVF leads, delayed R wave progression in V1-V4 leads (Figure 1). Initial laboratory tests revealed mildly elevated troponin I 0,8 ng/ml (<0,5 ng/ml), increased creatinine 144 ?mol/l with estimated glomerular filtration rate (CKD-EPI) 31,6 ml/min/1,73 m? and creatinine clearance (Cockcroft-Gault) 39 ml/min.

Figure 1. Electrocardiogram.
Coronary angiography showed occlusion in the distal part of the left circumflex artery without other significant coronary arteries lesions (Figure 2 A). Several attempts of balloon angioplasty were performed but failed to significantly improve distal flow (Figure 2 B). Nevertheless, the patient’s hemodynamic was stabilized. She received dual antiplatelet therapy (DAPT) with acetylsalicylic acid 100 mg, clopidogrel 75 mg and heparin 7500 units BID subcutaneously in intensive care unit, which was subsequently replaced with rivaroxaban 15 mg QD. 6-hours levels of troponin I was 4,0 ng/ml.

Figure 2. Coronary Angiogram.
(A) Occlusion in the distal part of the left circumflex artery.
(B) After balloon angioplasty.
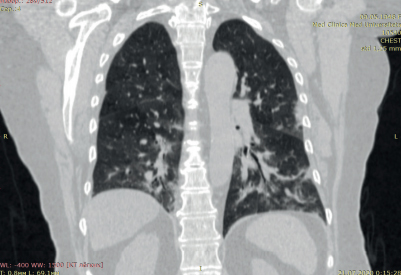
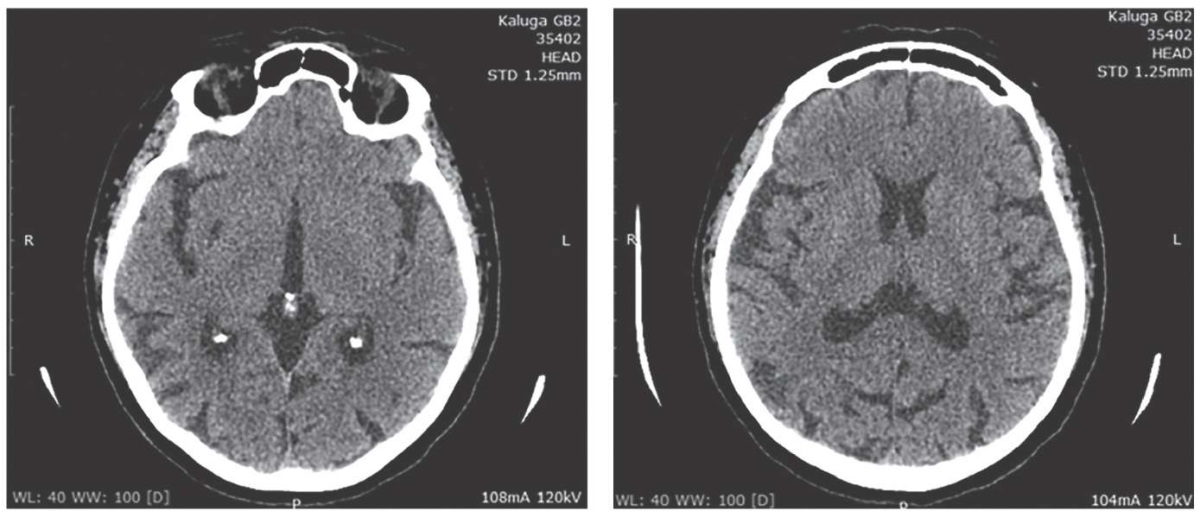
The same day performed brain computed tomography (CT) showed post-stroke cysts in the right temporoparietal region and the left cerebellar hemisphere (Figure 3). However, a hypodense focal area in the right temporal region suggesting an acute ischemic stroke was further diagnosed by magnetic resonance imaging (Figure 4). Ultrasonography of the brachiocephalic arteries showed a 40% stenosis of the left internal carotid artery.

Figure 3. Computed tomography showed post-stroke cysts.

Figure 4. Magnetic resonance imaging
showed hypodense focal area in the right temporal region.
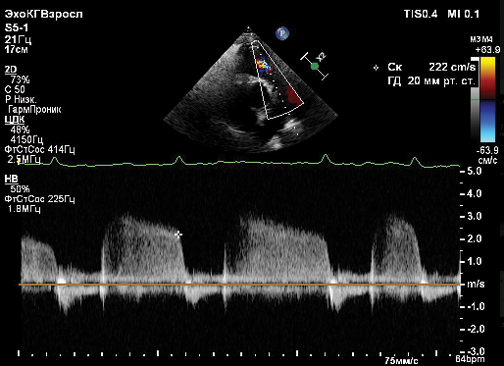
No significant changes were found on transthoracic echocardiogram besides enlarged left atrium (LAVI 48 mL/m?), mild left ventricular hypertrophy, ejection fraction (EF) was 67% without wall motion abnormalities. Transesophageal echocardiography to verify intracardiac thrombus was not performed due to technical reasons.
A week after admission the patient complained of a sudden onset of left upper quadrant abdominal pain, nausea and vomiting. Electrocardiography monitoring, cardiac biomarkers and additional lab tests were normal. A large hypodense focal area in the lower pole of the spleen suggesting a fresh splenic infarction was diagnosed by abdominal CT (Figure 5 A). Concomitant area of fibrosis (post infarct) in the middle third of the spleen, patches of postinfarct fibrosis in both kidneys and atherosclerosis of abdominal aorta were found (Figure 5 B).

Figure 5. Abdominal computed tomography.
(A) Splenic infarction,
(B) postinfarct fibrosis of both kidneys and in the middle third of the spleen.
Differential diagnosis
Sequential results obtained by multimodal visualization were very suggestive of AF-associated multisite embolism into coronary, brain, kidney, and splenic arteries. At the same time, the role of the significant aortic and carotid atherosclerosis and other factors predisposing to systemic thromboembolism such as cancer or thrombophilia was considered. No evidence of cancer was obtained during the diagnostic procedures. Testing for antiphospholipid antibodies was not performed due to inaccuracy in the results with ongoing anticoagulant therapy and clear inability to interrupt it, and negative family and personal history for thrombosis and/or pregnancy morbidity (the patient has 4 children). Moreover, in the setting of arterial thrombosis and stroke a recent guideline do not recommend testing for heritable thrombophilia due to a weak association between thrombophilias and arterial thrombosis (as opposed to venous thrombosis) [1].
Management
DAPT was stopped and rivaroxaban uptitrated up to 20 mg per day (creatinine clearance increased to 51 ml min). At 14th day of admission the patient remained well following her treatment and was discharged with no symptoms of angina or abdominal pain (CHA2DS2-VASc score-6, HAS-BLED score-3). Slight dysarthria persisted (NIHSS-1).
Discussion
AF is the most frequent cardiac arrhythmia associated with substantial risk of systemic thromboembolic events, cardiovascular morbidity and mortality [2-4]. Although stroke is the mostly considered serious complication of AF, extracranial embolic events accounted for only 11,5% and mainly involving lower extremities arteries (58%) have similar clinical and prognostic importance [5]. AF can be a reason for embolic MI in 3-13% of the cases and in 15% be associated with other emboliс events [6]. Simultaneous cardio-cerebral infarction and systemic embolic events are rare [7]. The incidence of acute renal infarctions and splenic infarctions is estimated to be 0,004-0,01% in hospitalized patients [8]. Importantly, some of the systemic embolism, such as renal microembolism, could be asymptomatic and presented only at the late stages of kidney disease, intuitively interpreted as a result of systemic atherosclerosis, significant comorbidities burden or ageing. Indeed, in the presented case of elderly women the involvement of cerebral, coronary and splenic arteries separately could be considered to be of atherosclerotic origin and ultrasound imaging revealed carotid stenosis, abdominal aortic atherosclerosis, and additionally occlusion of a small-diameter coronary artery could be due to plaque formation as well. Unfortunately, intravascular technics preferred for the latter scenario where coronary angiographic images do not visualize lumen segments adequately were not available. But simultaneous embolization of distinct vascular beds within 14 days and signs of previous organ infarctions suggested systemic AF-associated embolism caused by the lack of anticoagulant therapy. And what is remarkable, splenic infarctions developed on rivaroxaban.
Patients with AF and thromboembolic events should receive long-term oral anticoagulation with warfarin or direct oral anticoagulants unless there are contraindications [6][9]. However, to date there are no clear guidelines for, or clinical trials aimed at treatment of embolic MI due to AF. Available data are limited to case reports and few studies. Although thrombus aspiration is not recommended by the current MI guidelines (class of recommendations III) [10], this approach seems to be warranted and is considered as a primary strategy by some experts [9]. However, in 42% of patients with coronary embolism, similarly to our case, this is not feasible because of far distal occlusion or the small diameter of the artery [6] and the decision making regarding future conservative treatment is mainly left to the physicians’ opinion. In AF patients presented with acute coronary syndrome due to plaque rupture (i.e., type 1 MI), DAPT and full-dose anticoagulation should be administered [2]. In our case, coronary angiography showed occlusion in the distal part of the left circumflex artery without other significant coronary arteries lesions, which, along with embolism to other organs (brain, spleen, kidney), were very suggestive of coronary embolism as the cause of MI. Provided lack of evidence on optimal invasive and conservative strategies and given stenting of infarct-related artery was not performed, direct oral anticoagulant long-term monotherapy was recommended at discharge.
Follow-up
The patient remained clinically stable at 3-6-months follow-up visits of a cardiology outpatient clinic.
Conclusions
Systemic embolic events are rare complication of AF but could have acute symptomatic (MI, stroke, acute abdominal pain) and chronic silent consequences (heart failure, cognitive decline, chronic kidney disease). Patients with AF should be screen for indication and encouraged to start as early as possible and continue long-term oral anticoagulation unless there are contraindications. Optimal strategy for embolic MI is uncertain. Increasing burden of AF and associated systemic thromboembolic complications highlight the need of development of a consensus document for the diagnosis and treatment of embolic MI and further research in the field.
Relationships and Activities: none.

Чтобы читать статью войдите с логином и паролем от scardio.ru
Ключевые слова
Для цитирования
Новицкий Н.И., Багликов А.Н., Соловьева А.Е., Кручинова С.В., Космачева Е.Д., Виллевальде С.В. Идеальный шторм: клинический случай множественной (мозговой, коронарной, почечной и селезеночной) эмболии у пациента с фибрилляцией предсердий. Российский кардиологический журнал. 2023;28(3S):5472. https://doi.org/10.15829/1560-40712023-5472. EDN: RYDURC
Скопировать