Electrocardiographic parameters and features of ventricular arrhythmias in various arrhythmogenic cardiomyopathy forms in the pediatric population: a systematic review and meta-analysis
Аннотация
Arrhythmogenic cardiomyopathy (ACM) is a rare genetic disease characterized by the development of life-threatening ventricular arrhythmias and impaired ventricular systolic function due to fibrofatty infiltration of the myocardium. Currently, the Task Force 2010 criteria and the Padua criteria are proposed for the diagnosis of this disease. However, despite the multiparametric approach, there are certain limitations of the presented algorithms for disease establishment, especially in children. Carrying out such high-tech diagnostic methods as endomyocardial biopsy and magnetic resonance imaging is extremely difficult in the pediatric population. In this regard, the study and application of electrocardiography becomes extremely relevant in children. In addition, there are no data on the features of ventricular arrhythmias in ACM in the pediatric population. In this systematic review with meta-analysis, we studied the features of ventricular arrhythmias and electrocardiographic parameters in various ACM types.
Arrhythmogenic cardiomyopathy (ACM) is a ge – netic disease characterized by impaired ventricular systolic function due to progressive fibrofatty replacement of normal heart tissue and associated with development of ventricular arrhythmias (VAs) [1][2]. Initially, it was regarded as a right-sided ventricular disease, which was reflected in its name: arrhythmogenic right ventricular (RV) dysplasia [3]. But later, biventricular (BV) and left-dominant types of the disease were recognized. In 2019, the working group of the Heart Rhythm Society adopted the common term of the disease as ACM and proposed updated recommendations for the diagnosis, risk stratification and treatment of this nosology [4][5]. In the presented systematic review, we will use the term ACM with its form in order to avoid confusion in terminology.
The first diagnostic criteria for right-dominant ACM form were proposed in 1994 (Task Force) [6]. The last revision of these criteria was performed in 2010. According to the International Task Force 2010 criteria, family history data, electrocardiography (ECG), echocardiography (EchoCG), magnetic resonance imaging (MRI), 24-hour ECG monitoring, histological and genetic examinations are evaluated [7]. All criteria are divided into major and minor, depending on their specificity for the disease. To make a diagnosis, it is enough to have 2 major criteria, or 1 major and 2 minor criteria, or 4 minor ones. The diagnosis is considered possible in the presence of 2 minor criteria or 1 major, or 1 major and minor, or 3 minor criteria.
Despite the multiparametric approach, there are certain limitations of the presented diagnostic criteria. Thus, they do not allow assessment of other phenotypic variants other than RV dominance. A group of international experts pointed this out in 2019, and the updated Padua criteria were presented in 2020 [8, 9]. Currently, these criteria are not included in the recommendations for the diagnosis of ACM. According to these criteria, not only RV, but also LV involvement is taken into account. There are major and minor criteria and, depending on the quantitative correspondence, the diagnosis is considered definite, possible or borderline. Both EchoCG and MRI data are used as imaging methods in compliance with the Padua criteria. Unlike the Task Force 2010 criteria, where the sizes of the right heart chambers and ejection fraction values were indicated [7], the Padua criteria take into consideration the indexed dimensions of RV and LV cavities estimated by EchoCG and MRI taking into account body surface area, age, gender, and in accordance to the nomograms presented by the International Society for Cardiovascular Imaging [8]. There are certain difficulties in disease establishment of ACM, especially in the left-dominant form [10]. Thus, neither the Task Force 2010 nor the Padua criteria took into account the possibilities of diagnostic search in pediatric population. Complexities of the diagnosis of various ACM forms in children have been noted by many authors [11-13]. The absence of individual criteria for children with ACM complicates the diagnosis in pediatric practice. In addition, the questions of the originality of the clinical course of various ACM forms remain unclear.
ECG changes often precede morphological myocardial remodeling and make the diagnosis of ACM suspected. However, the use of ECG criteria is very limited in pediatric practice due to age characteristics. In particular, certain difficulties are caused by the interpretation of changes in the repolarization processes in children. Inverted T-wave in the right precordial leads V1-3 on ESG is a major criterion and is considered the most common, sensitive, and specific marker. It is generally recognized that this parameter is a normal phenomenon in pediatric patients under the age of 14 [14][15]. The Epsilon wave as the major criterion of the disease in conformity with the Task Force 2010 criteria is observed in the right precordial leads and is a characteristic feature of ACM, and corresponds to a delay in depolarization of the RV free wall and the outflow tract. It occurs predominantly in advanced cases of ACM and is extremely rare in children and adolescents [16, 17]. All this potentially leads to the exclusion of two important ECG criteria in the diagnosis of ACM in the pediatric population. The presence of late potentials (minor criterion) is also not typical in pediatric patients [16].
In addition, the implementation of such hightech diagnostic methods as endomyocardial biopsy and MRI is extremely arduous in the pediatric population. In this regard, the study of ECG features of ACM in children becomes extremely relevant in the diagnosis of this disease, which is primarily driven by the availability, ease of use and safety of these examination methods.
Moreover, the lack of data on the features of ventricular arrhythmias and ECG parameters in various phenotypic ACM types in the pediatric population prompted this systematic review with meta-analysis.
Thus, the objective of this systematic review with meta-analysis was to study the features of ventricular arrhythmias and electrocardiographic parameters in various ACM forms in pediatric patients.
Material and methods
Search for publications and selection of studies. The systematic review and meta-analysis were performed in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement. The search was carried out in the PubMed electronic database without restrictions on the date of issuing of publications and ended on March 8, 2022. Three independent investigators separately searched and selected studies using predefined search terms, keywords (including MeSH) and logical operators: “arrhythmogenic cardiomyopathy” and “Padua criteria” and “children” or “Phenotype” and “arrhythmogenic cardiomyopathy” and “children” or “right ventricular arrhythmogenic dysplasia and pediatric population”. Any disagreements were resolved through discussion between them or with the involvement of a fourth researcher, if the disagreement persisted. The search was limited to English-language articles. We included studies that 1) compared ECG parameters and features of VAs in pediatric patients with various phenotypic ACM forms; 2) described ECG signs and features of VAs in confirmed ACM in children. The studies representing animal trials, abstracts, minutes of meetings, books, clinical cases and case series were excluded. The eligibility of each work being included was checked in 2 steps: 1) review of the title and abstract, and 2) review of the full text.
Research data extraction and synthesis. The following data were recorded for each study: first author, year of publication, study population, number of cases, age of ACM onset, gender and the ensuing features based on Task Force 2010 or the Padua criteria: changes in the processes of depolarization and repolarization (inverted T-wave in the right precordial leads (V1-3), Epsilon wave in the right precordial leads (V1-3), late ventricular potentials, delayed intraventricular conduction, etc.), VAs and their morphological characteristics. Any disagreements were resolved through discussion.
Statistical analysis. Data meta-analysis was carried out using the free Open Meta-Analyst software. Given the significant statistical heterogeneity of most parameters, a random effects model was used when the data from individual studies summarized. Percentages with 95% confidence intervals (CI) were calculated using the Der Simonian-Laird method [18]. The results of meta-analysis were presented as a blobbogram (forestplot).
Comparison of the data of dominant-right ACM to BV and dominant-left types was performed by calculating the generalized frequency of pathological conditions with a preliminary addition of the number of cases and the number of patients studied in separate publications. Next, the statistical significance of differences in parameters was assessed using Pearson’s chi-square test, and the odds ratio with 95% CI was calculated. Differences were considered statistically significant at p<0,05.
Results
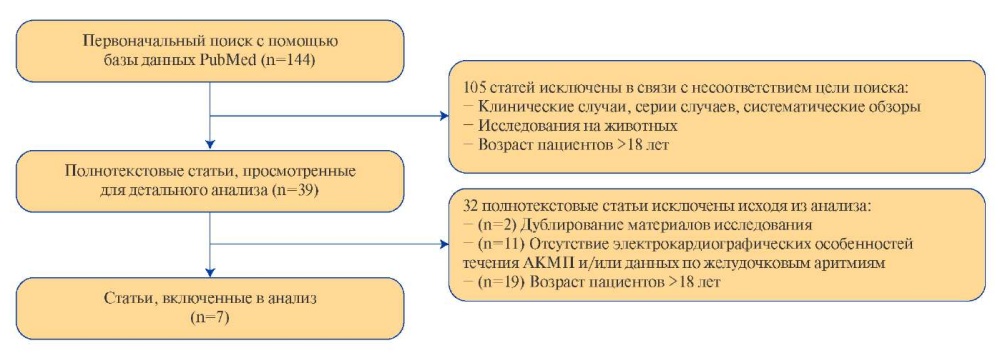
The initial electronic search identified 144 studies. In total, 39 papers remained after the removal of duplicated articles, clinical cases, studies on patients over the age of 18. Three independent researchers reviewed the full-text versions of the remaining publications and identified 5, 7, and 9 articles, respectively. Seven articles were selected for analysis after a collegial discussion and the involvement of the fourth researcher. The search algorithm is shown in Figure 1.
The number of children in 7 studies included in the analysis varied from 17 to 75; follow-up period varied from 1 year to 33 years.
We were unable to conduct a meta-analysis of data on the frequency of VAs and ECG features in “non-classical” ACM forms because the information was provided in single studies. At the same time, the meta-analysis was performed for cases of right-dominant ACM and the overall frequency of cases of VAs and ECG signs. Table 1 shows the characteristics of the studies included in the analysis [17][19-24].
ECG features. ECG abnormalities as changes in the processes of repolarization and depolarization were described in 6 studies. The most frequently recorded ECG parameter of repolarization was inverted T-wave in leads V1-3, which was described in half of the patients (n=197, 50,8%). Wherein, the frequency of this criterion occurrence taking into account ACM forms was presented in 5 out of 6 studies and, regardless of the phenotypic variant, was observed in half of the cases both in patients with BV (55,6%) and right-dominant (50,3%) ACM.
Among the changes in the processes of depolarization, the late ventricular potentials were the most common ones (in 49 cases out of 124). Quantitative data on those ventricular potentials were presented in 3 studies, and only in patients with right-dominant ACM. The results of the meta-analysis of the prevalence of the late ventricular potentials based on ECG data are presented in Figure 2.
In accordance with the data obtained, the frequency of disclosure of the late potentials was 39,4% (95% CI: 30,9-48,0). The parameter had low heterogeneity (I2 =0%, p=0,486), ranging from 37,0 (Riele, 2015) to 52,9% (Daliento, 1995).
Data on changes in depolarization were presented in 3 papers. The number of patients with rightdominant ACM who had this sign was 71 ones, when a total number of analyzed patients were 103. The results of the meta-analysis are shown in Figure 3.
As follows from the obtained blobbogram, the prevalence of changes in depolarization varied from 60,9 (Riele, 2015) to 87,5% (DeWitt, 2016) in different studies featuring in significant heterogeneity (I2 =72,7%, p=0,026). The composite rate was 74,8% (95% CI: 58,3-91,3).
DeWitt (2016) presented data on the frequency of detection of depolarization changes in BV ACM. The parameter was of 66,7% (6 cases out of 9 studies), which corresponded to the frequency of the symptom in dominant-right ACM.
The Epsilon wave was rare and was described in 5 papers, which corresponds to 4,86%. The distribution of this symptom was presented in 4 studies depending on ACM form: it occurred in 5 (5,0%) patients with RV damage and in one (11,9%) with BV form.
The detailed description of the ECG features is presented in Table 2.
The comparison results of the frequency of changes in ventricular depolarization on ECG data in patients with right-dominant ACM with the parameter in BV form presented in the study by DeWitt (2016) are shown in Table 3. In accordance with the table, the frequency of depolarization changes was of 68,9% in right-dominant ACM based on the generalized data of 3 studies, and it was of 66,7% in BV ACM in compliance with the results of the study by DeWitt (2016). The values of the parameters were comparable (p=1,0).
Ventricular arrhythmia (VA). VAs were described in all the papers included in the systematic review, however, their quantitative characteristics are presented in 6 ones. Data on the frequency of this symptom in any ACM form are presented in Table 4.
Thus, VAs were registered in 126 out of 210 (60,0%) patients, i.e. in more than half of the cases. In the meta-analysis, the overall incidence of VAs was of 61,4% (95% CI: 37,0-85,7). The data were highly heterogeneous (I2 =95,6%, p<0,001).
The proportion of identified ventricular tachycardia (VT) was of 46,7% in the meta-analysis of the studies on ACM of any localization including non-sustained ventricular tachycardia of 28,2%, and sustained VT of 22,9%.
According to the study by DeWitt (2016), VA was characteristic of all patients with both left-dominant and BV forms. Whereas, in the “classic” form of the disease described in 5 publications, VAs occurred in 101 out of 173 cases. The results of the meta-analysis of the frequency of VA in right-dominant ACM are presented in Figure 4.
The blobbogram above shows that the total proportion of patients with VAs was of 6,6% (95% CI: 34,6-9,6) in right-dominant ACM. The parameter, as well as in the analysis of ACM of any localization, was highly heterogeneous (I2 =95,6%, p<0,001).
Holter monitoring was performed in all studies. However, data on the quantitative characteristics of ventricular ectopic complexes >500 per day were presented only in 2 papers out of 7 and were described in the vast majority of children 55 (77,5%). Four studies showed the morphological characteristics of the VAs. Based on the data presented, enumeration was only possible in 3 studies.
Thus, VAs were registered in a third of patients as left bundle-branch block in 35,2% of cases and much less frequently as right bundle-branch block in 8,79% of cases. The correct numerical characteristic of the VT morphology was described in one paper presented only right-dominant ACM form. Thus, VT with the morphology of left bundlebranch block with the lower axis was recorded in 5 (9,43%) patients, and left bundle-branch block with the upper axis was registered in 4 (7,55%) patients.
When assessing the frequency of VT in patients with right-dominant ACM, this symptom was observed in 91 patients out of 173. As the result of the meta-analysis, the following blobbogram was obtained (Figure 5).
According to the data obtained, the incidence of VT was of 48,3% (95% CI: 24,3-72,3) in patients with right-dominant ACM. The parameter was highly heterogeneous (I2 =91,1%, p<0,001), ranging from 30,4% (Etoom, 2015) to 79,7% (Riele, 2015).
Non-sustained VT was observed in 18 out of 86 cases in right-dominant ACM. The results of the meta-analysis of this parameter are presented in Figure 6.
The meta-analysis of 3 studies found that the incidence of non-sustained VT was of 20,1% (95% CI: 11,7-28,5). The parameter had a insignificant heterogeneity (I2 =0%, p=0,562), which corresponded to close values of the frequency of nonsustained VT in right-dominant ACM obtained by different researchers: from 12,5% (DeWitt, 2016) to 23,5% (Daliento, 1995).
Eventually, sustained VT in right-dominant ACM was observed in 24 patients out of 145 described in 3 studies. Based on the results of the meta-analysis, the following blobbogram was obtained (Figure 7).
The reported rate was of 15,4% (95% CI: 6,9- 23,9). The range of values corresponding to different studies accounted from 9,4 to 21,3%, the parameter was moderately heterogeneous (I2 =47,2%, p=0,15).
We also compared the frequency of VA, VT, and non-sustained VT depending on the phenotypic forms of ACM. As in previous cases, data on the frequency of these conditions for left-dominant and BV ACM were taken from the study by DeWitt (2016). The results obtained are reflected in Table 5. This table shows that the frequency of VA in patients with the left-dominant and BV ACM forms, reaching 100% in both cases, was significantly higher than in those with right-dominant ACM, which was of 58,4% (p=0,043 and p=0,012, respectively). On the contrary, the rate of VT was higher in right-dominant ACM (up to 52,6%), whereas the rate was of 42,9% in left- dominant ACM, and it was of 22,2% in the BV form. Despite the fact that the incidence of VT was over twofold higher in the right-dominant form than in the BV form, the difference was not statistically significant (p=0,095). There were also no statistically significant differences between left-dominant and rightdominant ACM (p=0,711).
In the analysis of the frequency of non-sustained VT, right-dominant ACM form this symptom was found to occur only in 20,9% of the subjects. Among patients with a left-dominant form of the disease, the incidence of non-sustained VT was almost threefold higher, up to 57,1%, and it was 3,7-fold higher in BV ACM patients, up to 77,8%. The differences were characterized by p=0,052 when comparing rightdominant and left-dominant ACM forms, which suggests a certain relationship between the morphological forms of ACM and the frequency of non-sustained VT. The parameter statistically significantly exceeded the frequency of non-sustained VT in BV ACM than in right-dominant ACM (p=0,001).
Thus, a significantly higher incidence of VA in general, as well as non-sustained VT, was found in patients with left-dominant and BV ACM forms compared to dominant-right ACM.

Figure 1. Selection algorithm of publications.
Abbreviation: ACM — arrhythmogenic cardiomyopathy.

Figure 2. The meta-analysis of the frequency of late potentials on ECG in patients with right-dominant ACM.
Abbreviation: CI — confidential interval.
Table 1
Studies included in the systematic review

Abbreviations: ACM — arrhythmogenic cardiomyopathy, BV — biventricular, LD — left-dominant, DR — right-dominant.

Figure 3. The meta-analysis of the frequency of depolarization changes on ECG in patients with right-dominant ACM.
Abbreviation: CI — confidential interval.
Table 2
ECG features in patients included in the systematic review

Abbreviations: BV — biventricular, LD — left-dominant, DR — right-dominant.
Table 3
The comparison results of the frequency of changes in ventricular depolarization on ECG in various ACM forms

Abbreviations: BV — biventricular, RD — right-dominant.
Table 4
The frequency of VA in ACM of any localization

Abbreviations: CI — confidential interval, VA — ventricular arrhythmias, VT — ventricular tachycardia.

Figure 4. The meta-analysis of the frequency of VA in patients with right-dominant ACM.
Abbreviation: CI — confidential interval.

Figure 5. The meta-analysis of the frequency of VA in patients with right-dominant ACM.
Abbreviation: CI — confidential interval.

Figure 6. The meta-analysis of the frequency of non-sustained VT in patients with right-dominant ACM.
Abbreviation: CI — confidential interval.

Figure 7. The meta-analysis of the frequency of sustained VT in patients with right-dominant ACM.
Abbreviation: CI — confidential interval.
Table 5
The comparison results of the frequency of VA in various ACM forms

Note: * — statistically significant differences (p<0,05).
Abbreviations: BV — biventricular, VA — ventricular arrhythmias, VT — ventricular tachycardia, LD — left-dominant, DR — right-dominant.
Discussion
Our systematic review with meta-analysis demonstrates the features of VA and ECG parameters in children with various ACM forms, and also gives a general idea of the characteristics of the above parameters.
More than half of the patients had VA. Wherein, compared to right-dominant ACM, the number of patients with VAs significantly prevailed in “nonclassical” one. A significantly higher incidence of non-sustained VT was also established in patients with left-dominant and BV ACM forms than in those with right-dominant ACM. However, as per literature, VA is the main manifestation of ACM, regardless of the phenotype [25][26].
ECG criteria of the disease are known to include both changes in the processes of depolarization and repolarization. At the same time, their relevance in the diagnosis of only right-dominant and BV forms should be taken into account.
The results of this work revealed that the change in depolarization such as the Epsilon wave is quite rare, regardless of the ventricle involvement. Our conclusions correlate with the literature data: the Epsilon wave is extremely rare, mainly in the late stages of the disease, and the detection of the Epsilon wave on ECG is a minor criterion in the updated Padua criteria [4, 27]. This is probably due to the fact that this sign manifests itself at later stages of the disease, when there is a significant structural pathology of the heart [7][28]. In addition, it is known that this pattern on the ECG may be transient and not manifest during repeated examinations [29]. The late ventricular potentials have been described to also depend on the progression of the disease, but they are much more common than the Epsilon wave [16]. So according to our data, the late ventricular potentials were recorded in more than a third of cases with right-dominant form. In addition, the frequency of depolarization changes in both right-dominant and BV forms did not differ significantly and was observed in a significant number of patients. This observation is warranted further research and study of this phenomenon.
Among the repolarization changes, the most common, sensitive and specific marker is inverted T-wave in the right precordial leads V1-3, which is a major diagnostic criterion for ACM. It should be noted that this criterion cannot be used in children under 14 years of age, because it is the age norm [14][15]. In our study, these changes were described in more than a third of patients, but, unfortunately, they did not carry any diagnostic value, because the average age of the children included in the study was of 13,5 years.
Thus, our systematic review with meta-analysis concludes that VA is the leading sign of ACM in the pediatric population. Wherein, non-sustained VT is recorded much more often in “non-classical” forms than in right-dominant ACM. Among the ECG parameters that should be paid attention to in children, one can single out the changes in depolarization processes. At the same time, the late ventricular potentials can be considered as a promising diagnostic criterion for RV involvement in children.
Study limitations. Our study has several limitations. ECG parameters were not clearly presented in most cases, which made it difficult to perform the meta-analysis in many ways. The heterogeneity in the range of the described VA characteristics should be noted as a complication of the analysis.
Conclusion
The publications included in our systematic review with meta-analysis demonstrated the promising prognostic value of a number of ECG parameters. Taking into account the absence of specific ECG signs in children, it is necessary to provide dynamic monitoring of patients with VAs and continue further research to study the ECG parameters and features of VA in order to develop diagnostic criteria for ACM in the pediatric population.
Relationships and Activities. The study was financially supported by the Ministry of Science and Higher Education of the Russian Federation (Agreement № 075-15-2022-301 dated April 20, 2022).

Чтобы читать статью войдите с логином и паролем от scardio.ru
Keywords
For citation
Alekseeva D.Yu., Kofeynikova O.А., Marapov D.I., Vasichkina E.S. Electrocardiographic parameters and features of ventricular arrhythmias in various arrhythmogenic cardiomyopathy forms in the pediatric population: a systematic review and meta-analysis. Russian Journal of Cardiology. 2022;27(3S):5147. https://doi.org/10.15829/1560-4071-2022-5147
Copy