Efficacy and safety of combined aspirin and warfarin therapy after heart valve replacement: a systematic review and meta-analysis of randomized clinical trials
Аннотация
Aim. To conduct a systematic review and meta-analysis of the efficacy and safety of combined oral anticoagulant therapy with vitamin K antagonists (VKA) and antiplatelet therapy with aspirin compared with VKA monotherapy in patients after mechanical valve replacement.
Material and methods. We searched the PubMed, Google Scholar databases for studies comparing the risk of thromboembolic events, major bleeding, and mortality in VKA monotherapy versus combined aspirin and VKA therapy in patients with mechanical valve replacement.
Results. Eight randomized clinical trials were selected for this systematic review and meta-analysis. In total, 4082 patients were included in the analysis (mean age, 50,8 years, men — 2484 (60,9%)). A meta-analysis showed that the addition of aspirin to VKA, compared with VKA monotherapy, significantly reduced the incidence of thromboembolic events (odds ratio (OR) 0,47; 95% confidence interval (CI): 0,33-0,67; p<0,0001) and mortality (OR 0,58; 95% CI: 0,38-0,88; p=0,01). The risk of major bleeding in the aspirin plus VKA group compared with VKA monotherapy tended to increase, without reaching a significant difference (OR 1,41; 95% CI: 0,99-2,01; p=0,06). Conclusion. The addition of aspirin to VKA, compared with VKA monotherapy, reduces the risk of systemic embolism and death in patients after mechanical valve replacement. At the same time, the risk of major bleeding did not differ between the groups.
Ischemic and nonischemic cardiomyopathies are currently the main causes of chronic heart failure (HF) with reduced left ventricle (LV) ejection fraction (EF) [1]. It is associated with significant morbidity and premature mortality, primarily, due to the development of decompensated HF and sudden cardiac death (SCD) [1][2]. The current risk stratification criteria are far from being perfect. There is a need for new risk stratification tools, since the majority of patients who, in particular, are implanted with the cardioverter-defibrillator for primary prevention of SCD, do not experience motivated device activations [3].
The emergence of myocardial deformation estimation methods by the technology of tracking the movement of gray scale spots in a two-dimensional image (speckle tracking echocardiography (STE)) made it possible to assess early ventricular dysfunction in the absence of obvious structural changes in the myocardium [4]. Over the past decade, there has been an increasing number of studies on the role of left ventricular global longitudinal strain (LV GLS) estimated by 2D STE to predict adverse events in patients with HFrEF [5]. Most of these studies have shown that deterioration of LV GLS is associated with the development of adverse cardiovascular events. It should be noted that not only LV GLS, but also left ventricular mechanical dispersion (LV MD) has proved to be a surrogate marker of delayed and inhomogeneous conduction in the myocardium and has been associated with the risk of arrhythmic events both in ischemic and nonischemic cardiomyopathy [6]. However, the use of these new echocardiographic markers is currently limited to only small, single-centre, observational clinical trials with little sample sizes and few events.
In light of these shortcomings, a systematic review and meta-analysis of studies on the prognostic role of LV GLS and MD in patients with ischemic and nonischemic cardiomyopathy were carried out.
Material and methods
Search for publications and selection of studies. The information retrieval algorithm was developed in accordance with the reporting requirements and regulations for systematic reviews and meta-analyses (PRISMA) [7] in the PubMed, Google Scholar and EMBASE databases. The last data search for inclusion in this analysis was performed on February 4, 2022. We used the following keywords to search PubMed and EMBASE databases: ((dilated cardiomyopathy) OR (non-ischemic dilated cardiomyopathy) OR (ischemic dilated cardiomyopathy) OR (Heart Failure)) AND ((Echocardiography) AND (speckle tracking) OR (Strain) OR (Global Longitudinal Strain) OR (Myocardial strain) OR (dyssynchrony) OR (dispersion)) AND ((risk assessment) OR (predictive value) OR (prognostic value)). The following query was used to search the Google Scholar database: speckle tracking echocardiography, Global Longitudinal Strain, dispersion, Nonischemic Dilated Cardiomyopathy, Ischemic Dilated Cardiomyopathy, Heart Failure, prognostic value, hazard ratio cox regression.
Two authors independently reviewed abstracts and full-text articles for inclusion criteria to select eligible studies for this systematic review and metaanalysis.
Inclusion/exclusion criteria. The inclusion criteria of primary studies in a systematic review followed by meta-analysis were: the access to full-text studies; all participants were adults (18 years or over); the studies with adequately presented baseline data, mainly data on the longitudinal strain and/or LV MD values measured by STE. In addition, the mandatory criteria to include publication in the metaanalysis were both the data on clinical outcomes and the results of univariate and/or multivariate Cox regression analysis with hazard ratio (HR). The lower observation period threshold of patients was set at 12 months (the average period). The articles in languages other than English, case reports, preclinical studies, reviews, and expert opinions were excluded from the meta-analysis.
Assessment of the methodological quality. The quality of the studies was evaluated on NewcastleOttawa quality assessment scale [8]. The evaluation of studies was carried out based on of the following main criteria: selection of research groups; group comparability; and setting the outcome of interest. All inconsistencies were eliminated by authors’ discussion of this work.
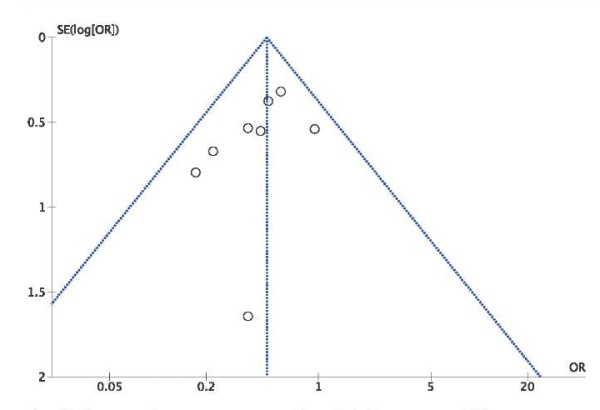
Statistical analysis. Statistical data processing was performed using Review Manager (RevMan), version 5.4.1 (The Cochrane Collaboration, 2020) and Comprehensive Meta-Analysis 3.0 (Biostat, NJ). Meta-analysis was carried out according to the random effects model, using the inverse dispersion method. Graphically, the main results are presented in a “forest” diagram (forest plot). Statistical heterogeneity was assessed by Pearson’s chi-square test and heterogeneity index I2. Interpretation of the statistical heterogeneity assessment with the I2 index was carried out according to the recommendation of Cochrane Collaboration. A guide to interpretation of I2 index is as follows: 0% to 40% might not be important; 30% to 60% may represent moderate heterogeneity; 50% to 90% may represent substantial heterogeneity; 75% to 100% may represent considerable heterogeneity. The baseline values for metaanalysis of survival rates were used the unadjusted (obtained for a single-factor model) and adjusted (obtained for a multivariate model) HR, determined for changes in LV GGL and MD per 1% and 10 ms, respectively. Publication bias was assessed by the Egger test. The effect was considered statistically significant at p<0,05.
Results
Flowchart of literature review
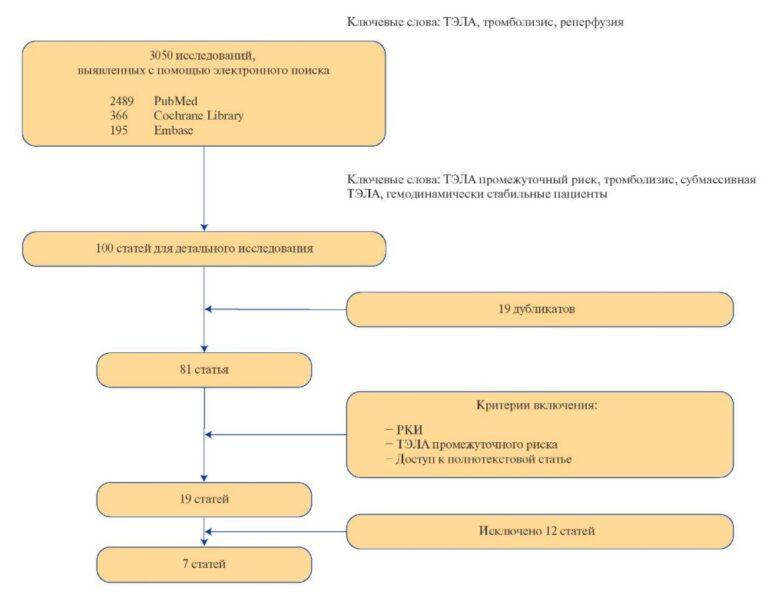
A total of 314 publications were found on the search results for those keywords in the PubMed, Google Scholar and EMBASE databases. The number of publications after the removal of duplicates was 302. Thirty seven publications corresponded to the goal after their titles and abstracts analyzed. The most common reasons to exclude an article were inconsistency with the goal and the lack of given data. The review articles, discussions, abstracts and reports were also excluded. Full-text screening of 20 publications was performed.
Three studies did not present comparative analysis of LV GLS parameters in patients with and without endpoints, or Cox regression analysis with calculated HR. Therefore these studies were excluded from our analysis [9-11]. In one study, LV GLS and MD were presented as binary data with a diagnostic cut-off values that prevented us to include this study for a pooled analysis of continuous data [12]. Another study presented highly heterogeneous groups of patients with hypertrophic cardiomyopathy and cardiac sarcaidosis, along with ischemic and nonischemic dilated cardiomyopathies, and therefore this study was also eliminated from our analysis [13]. Thus, 12 studies were finally included in our review; Figure 1 shows the selection process for relevant studies.
General characteristics of studies
In total, 2624 patients with HFrEF caused by ischemic or nonischemic cardiomyopathies were enrolled in this analysis. All patients underwent assessment of LV GLS and/or MD by STE. The mean age of the patients was of 57,9 years. The mean follow-up period was of 40,8 months. Data on study design, baseline patient characteristics are summarized in Table 1.

Figure 1. Study selection flowchart.
Table 1
Summary of studies included in the systematic review

Abbreviations: CAD — coronary artery disease, ICM — ischemic cardiomyopathy, NICM — nonischemic cardiomyopathy, LV EF — left ventricle ejection fraction, NR — not reported.
Echocardiography data
The echocardiography data were obtained on expert-class ultrasound device (General Electric, Philips, Siemens and Toshiba). In most studies (8 publications) the data were post-processed on EchoPAC workstations (GE), in one study the data were obtained on TomTec workstations (TomTec Imaging Systems) [19], in one study the data were evaluated on Syngo Dynamics 9.0 software machine (Siemens) [15], and in one more study the data were assessed on 2DST software (Toshiba Medical Systems) [20]. LV GLS was evaluated by 2D STE technology. The main characteristics of echocardiographic equipment and software are presented in Table 2.
Endpoints and adverse outcomes
The main endpoints in studies assessing LV GLS and/or MD were “arrhythmic” events (5 studies) [14][18][19][21][25], major cardiovascular adverse events (MACEs) (5 studies) [15][16][20][22][24] and reverse LV remodeling (1 study) [23].
The “arrhythmic” endpoints included a variety of events (sustained ventricular tachycardia, ventricular fibrillation, implantable cardioverter-defibrillator motivated activations, SCD). Most of the studies presented a composite endpoint defined as cardiovascular death, heart transplantation, hospitalization for decompensated heart failure, or implantation of LV mechanical support devices. We calculated the totality of these events as large MACEs for the further meta-analysis. Most of the studies enrolled in our analysis presented data on LV GLS [14-17][19-25], three studies [14][16][21] also reported on LV MD, and in one study [18] only LV MD values were assessed. Table 3 presents the main values of GLS and LV MD parameters, as well as data on endpoints and the number of events in each group. Tables 4 and 5 show the HRs for the endpoint development obtained as a result of univariate and multivariate regression analysis by the Cox method after the inclusion of continuous variables such as LV GLS and/or LV MD values as predictors. Studies where a similar score criterion (changes in LV GLS and LV MD per 1% and per 10 ms, respectively) was available by endpoint were pooled together in a meta-analysis.
Table 2
Characteristics (specification) of ultrasonic equipment used in research

Abbreviation: NR — not reported.
Table 3
LV strain and MD indices included in the systematic review of publications

Abbreviations: SCD — sudden cardiac death, GLS — global longitudinal strain, VT — ventricular tachycardia, ICD — implantable cardioverter-defibrillator, LV — left ventricle, MD — mechanical dispersion, HF– heart failure, VF — ventricular fibrillation.
Table 4
Estimated changes of LV GLS and MD with the HRs calculated from the univariate Cox regression model

Abbreviations: CI — confidence interval, GLS — global longitudinal strain, LV — left ventricle, MD — mechanical dispersion, HR — hazard ratio, MACE — major adverse cardiovascular event, SE — standard error.
Table 5
Estimated changes of LV GLS and MD with the HRs calculated from the multivariate Cox regression model

Abbreviations: MRA — mineralocorticoid receptor antagonists, LBBB — left bundle-branch block, ARB — angiotensin II receptor blockers, GLS — global circumferential strain, GSC — global circumferential strain, CI — confidence interval, iACE — angiotensinconverting enzyme inhibitors, EDV — end-diastolic volume, EDD — end-diastolic dimension, ESD — end-systolic dimension, LV — left ventricle, LA — left atrium, MD — mechanical dispersion, HR — hazard ratio, CRT-D — cardiac resynchronization therapy defibrillator, LV — left ventricle, FC — functional class, BNP — B-type natriuretic peptide, MACE — major adverse cardiovascular event, NYHA — New York Heart Association, SE — standard error, SD — standard deviation.
The “arrhythmic” endpoint
Mean values of LV GLS depending on the “arrhythmic” endpoint development were presented in five studies. We performed a meta-analysis of the difference between the mean values of LV GLS in patients with and without the “arrhythmic” endpoints (Figure 2). Figure 2 shows that patients with ventricular arrhythmias (VA) had worse LV GLS values than those without it, so the weighted mean difference in LV GLS values was of 3,12% (95% confidence interval (CI): -5,13, -1,11%), these differences were statistically significant (p=0,002). The Egger test score were found to be statistically negligible, t=1,37; df=3,0; p=0,26.
A meta-analysis was also performed on the difference between the mean values of LV MD in patients with and without the “arrhythmic” endpoints (Figure 3). Figure 3 presents that patients with the arrhythmic endpoint had greater LV MD values compared to patients without it, so the weighted mean difference of LV MD was of 33,69 ms (95% CI: -41,32; -26,05), these differences were statistically significant (p<0,0001). The Egger test score were also found to be statistically negligible, t=1,08; df=1,0; p=0,48.
The univariate risk analysis data of the “arrhythmic” endpoints using continuous estimates of the LV GLS value as a predictor were presented in three studies [14, 17, 21]. These studies were comparable due to the same predictor score (changes per 1%), and that allowed to performed a meta-analysis of these publications. The number of the “arrhythmic” endpoints in these studies was of 96 (17,2% of 558 patients), the average follow-up period was of 29,8 months. In a pooled analysis, the deterioration of LV GLS was associated with a statistically significant increase in the weighted average risk of the VA development (HR: 1,17 per each 1% of LV GLS deterioration; 95% CI: 1,07-1,27; p=0.0005) (Figure 4). The Egger test score were also found to be statistically negligible, t=0,63; df=2,0; p=0,59.
The univariate risk analysis data of the VA development using continuous estimates of LV MD value as a predictor were presented only in two studies when [14][21]. These studies were comparable due to the same predictor score (changes per 10 ms), that allowed to performed a meta-analysis of these publications. The number of the “arrhythmic” endpoints in these studies was of 60 (13,8% of 434 patients), the average follow-up period was of 29 months. In a pooled analysis, an increment of LV MD was associated with a statistically significant increase in the weighted average risk of the VA development (HR: 1,29 per each 10 ms of LV MD increment; 95% CI: 1,14-1,47; p<0,0001) (Figure 5).
The multivariate risk analysis data of the “arrhythmic” endpoint development using continuous estimates of the LV GLS value as a predictor were presented in four studies [14][17][21][25]. These studies were comparable due to the same predictor score (changes per 1%), that allowed to perform a meta-analysis of these publications. The number of the “arrhythmic” endpoints in these studies was of 128 (15,1% of 848 patients), the average follow-up period was of 31,4 months. In a pooled analysis, LV GLS deterioration was associated with a statistically significant increase in the weighted average risk of the VA development (adjusted HR: 1,10 per each 1% decline of LV GLS; 95% CI: 1,01-1,19; p=0,03) (Figure 6). The Egger test score were also found to be statistically negligible, t=2,82; df=2,0; p=0,106.
The multivariate risk analysis data of the “arrhythmic” endpoint development using continuous estimates of the value of LV MD as a predictor were presented in three studies [14][21][25]. These studies were comparable due to the same predictor score (changes per 10 ms), that allowed to carry out a meta-analysis of these publications. The number of the “arrhythmic” endpoints in these studies was of 92 (12,7% of 724 patients), the average follow-up period was of 26,6 months. In a pooled analysis, the increase of LV MD was associated with a statistically significant increment of the weighted average risk of the VA development (adjusted HR: 1,18 per each 10 ms of LV MD increase; 95% CI: 1,08-1,29; p=0,0002) (Figure 7).
Major adverse cardiovascular events
Mean values of LV GLS parameters depending on the MACE development were presented in 5 studies. We performed a meta-analysis of the difference between the mean values of LV GLS in patients with and without MACE (Figure 8). Patients with MACE had worse LV GLS compared to those without it, so the weighted mean difference in LV GLS values was of -3,15% (95% CI: -4,27; -2,03%), these differences were statistically significant (p<0,0001).
The univariate risk analysis data of MACE development using continuous estimates of LV GLS as a predictor were presented in four studies [15][20][22][24] (Table 4). A similar score criterion (changes per 1%) was available in these studies, that allowed them to be pooled in a meta-analysis. In these studies, 144 patients experienced MACEs (31,7% of 454). The mean follow-up period was of 45,7 months. According to the results of the analysis, there was no statistically significant association between the LV GLS deterioration and the development of MACEs (HR: 1,17 per each 1% of LV GLS deterioration; 95% CI: 0,96-1,41; p=0,11) (Figure 9). The Egger test score were also found to be statistically negligible, t=0,48; df=2,0; p=0,67. It should be noted that the results of the meta-analysis were associated with the Santos’ study inclusion, 2019 [22], where conflicting data were presented. Thus, it was shown that LV GLS deterioration was associated with a decrease in the rate of MACE development according to one-way analysis (HR: 0,879; 95% CI: 0,784-0,985; p=0,026). At the same time, according to multivariate analysis, LV GLS decline was associated with an increased risk of MACE development (adjusted HR: 1,365; 95% CI: 1,106-1,686; p=0,003).
Therefore, we excluded the Santos’ study, 2019 [22] from the further meta-analysis. In the studies that were subsequently pooled [15][20][24], the MACE endpoint was reached in 138 patients (33,3% of 414). The mean follow-up period was of 55,0 months. A meta-analysis showed that LV GLS deterioration was associated with a statistically significant increase in the weighted average risk of MACE development (unadjusted RR: 1,27 per each 1% of GLS decline; 95% CI: 1,11-1,46; p=0,0008) (Figure 10). The Egger test score were found to be statistically negligible, t=5,8; df=1,0; p=0,11.
The multivariate risk analysis data of MACE development using continuous estimates of the LV GLS values as a predictor were presented in four studies [15][20][22][24]. These studies were comparable due to the same predictor score (changes per 1%), that allowed to carry out a meta-analysis of these publications. In these studies, the MACEs were registered in 144 patients (31,7% of 454). The mean follow-up period was of 45,7 months. In a pooled analysis, LV GLS deterioration was associated with a statistically significant increase in the weighted average risk of MACE (adjusted RR: 1,22 for each 1% worsening of LV GLS; 95% CI: 1,11-1,33; p<0,0001) (Figure 11). The Egger test score were also found to be statistically negligible, t=1,73; df=2,0; p=0,22.

Figure 2. Results of a meta-analysis of the difference between the mean LV GLS values in the group with VAs and without it.
Note: the green squares show weighted effect sizes for each specific study (the green square sizes represent weights of studies), the black line segments show 95% CI, the black rhombus shows weighted average of GLS mean difference. The color figure is available in the electronic version of the journal.
Abbreviations: GLS — global longitudinal strain, CI — confidence interval, VA — ventricular arrhythmias.

Figure 3. Results of a meta-analysis of the difference between the mean LV MD values in the group with VAs and without it.
Note: the green squares show weighted effect sizes for each specific study (the green square sizes represent weights of studies), the black line segments show 95% CI, the black rhombus shows weighted average of GLS mean difference. The color figure is available in the electronic version of the journal.
Abbreviations: MD — mechanical dispersion, CI — confidence interval, VA — ventricular arrhythmias.

Figure 4. Results of a meta-analysis of the unadjusted HR for “arrhythmic” endpoints per each 1% decline of LV GLS.
Note: the red squares show the weighted effect size for each particular study (the red square sizes represent weights of studies), the red line segments show 95% CI, the black rhombus shows weighted average of HR. The color figure is available in the electronic version of the journal.
Abbreviations: CI — confidence interval, HR — hazard ratio.

Figure 5. Results of a meta-analysis of the unadjusted HR for “arrhythmic” endpoints per each 10 ms increment of LV MD.
Note: the red squares show the weighted effect size for each particular study (the red square sizes represent weights of studies), the red line segments show 95% CI, the black rhombus shows weighted average of HR. The color figure is available in the electronic version of the journal.
Abbreviations: CI — confidence interval, HR — hazard ratio.

Figure 6. Results of a meta-analysis of the adjusted HR for “arrhythmic” endpoints per each 1% decline of LV GLS.
Note: the red squares show the weighted effect size for each particular study (the red square sizes represent weights of studies), the red line segments show 95% CI, the black rhombus shows weighted average of HR. The color figure is available in the electronic version of the journal.
Abbreviations: CI — confidence interval, HR — hazard ratio.

Figure 7. Results of a meta-analysis of the adjusted HR for “arrhythmic” endpoints per each 10 ms increment of LV MD.
Note: the red squares show the weighted effect size for each particular study (the red square sizes represent weights of studies), the red line segments show 95% CI, the black rhombus shows weighted average of HR. The color figure is available in the electronic version of the journal.
Abbreviations: CI — confidence interval, HR — hazard ratio.

Figure 8. Results of a meta-analysis of the difference between the mean LV GLS values in the group with MACEs and without it.
Note: the green squares show weighted effect sizes for each specific study (the green square sizes represent weights of studies), the black line segments show 95% CI, the black rhombus shows weighted average of GLS mean difference. The color figure is available in the electronic version of the journal.
Abbreviations: GLS — global longitudinal strain, CI — confidence interval, MACE — major adverse cardiovascular event.

Figure 9. Results of a meta-analysis of the unadjusted HR for MACEs per each 1% decline of LV GLS.
Note: the red squares show the weighted effect size for each particular study (the red square sizes represent weights of studies), the red line segments show 95% CI, the black rhombus shows weighted average of HR. The color figure is available in the electronic version of the journal.
Abbreviations: CI — confidence interval, HR — hazard ratio.

Figure 10. Results of a meta-analysis of the unadjusted HR for MACEs per each 1% decline of LV GLS (without Santos’ study, 2019).
Note: the red squares show the weighted effect size for each particular study (the red square sizes represent weights of studies), the red line segments show 95% CI, the black rhombus shows weighted average of HR. The color figure is available in the electronic version of the journal.
Abbreviations: CI — confidence interval, HR — hazard ratio.

Figure 11. Results of a meta-analysis of the adjusted HR for MACEs per each 1% decline of LV GLS.
Note: the red squares show the weighted effect size for each particular study (the red square sizes represent weights of studies), the red line segments show 95% CI, the black rhombus shows weighted average of HR. The color figure is available in the electronic version of the journal.
Abbreviations: CI — confidence interval, HR — hazard ratio.
Discussion
Nowadays, the current strategies of risk stratification in patients with chronic HF with reduced EF caused by ischemic or non-ischemic cardiomyopathy are far from being perfect. There is still a clinical need to identify new markers to help in risk stratification. LV EF is a global assessment of LV systolic function, which is not always associated with myocardial injury and electrophysiological disturbances underlying electrical myocardial instability. All mentioned above highlights the need to use other additional parameters for risk stratification.
At the time of this writing, we could not find published meta-analyses regarding the prognostic role of LV GLS in patients with ischemic and nonischemic cardiomyopathy.
In this article, the patients developed VAs and MACEs have been shown to possess statistically significantly LV GLS decline than those without it. In addition, LV GLS has been established to be an independent predictor of adverse arrhythmic events and MACEs. Thus, according to the results of the pooled analysis, LV GLS deterioration per each 1% has been shown to be associated with a statistically significant increase in the weighted average risk of the “arrhythmic” endpoint and MACE development by 10% and 22%, respectively.
As noted, LV MD is a marker of delayed and inhomogeneous conduction in the myocardium and can be used as a predictor of the VA development. A recent meta-analysis of 3198 patients by Kawakami and colleagues found that patients with VAs had higher LV MD values compared to those without it, so the weighted mean difference in LV MD values was of 20,3 ms (95% CI: 27,3-13,2; p<0,01). According to the results of the meta-analysis, each 10 ms increment of LV MD was associated with a statistically significant increase in the weighted average risk of VA development (adjusted HR: 1,19; 95% CI: 1,09-1,29; p<0,01). Moreover, the predictive value of LV MD was higher than the estimate of LV EF or LV GLS. It should also be noted that this meta-analysis included patients with both preserved and reduced LVEF, and most patients had prior myocardial infarction.
In our line of work, patients with ischemic and nonischemic cardiomyopathy with VAs have been established to have a statistically significantly higher LV DM values than those without “arrhythmic” endpoints. LV MD has also been shown to be an independent predictor of VA development. According to the results of the pooled analysis, each 10 ms increase of LV MD was associated with a statistically significant increase in the weighted average risk of “arrhythmic” endpoints by 18%. Thus, the assessment of LV GLS and LV MD by STE can be used as an effective tool for risk stratification in patients with HFrEF.
Study limitations. Firstly, a small number of studies were included in our systematic review and meta-analysis. Furthermore, as with any meta-analysis of observational studies, differences in inclusion criteria and endpoints are potential sources of study heterogeneity. Given the limited number of studies and patients, we are currently unable to perform a meta-analysis separately for groups with ischemic and nonischemic dilated cardiomyopathy, because some studies included a mixed population of patients with both types of cardiomyopathy and did not provide subgroup analysis data. Secondly, in the analysis we included the HR data obtained for LV GLS and/or LV MD, according to the data of both univariate and multivariate Cox regression analysis with calculated adjusted HR values.
However, in the latter case, the multivariate analysis included diverse covariates (age, gender, LV EF, LV end-diastolic volume, GPP, etc.) in various studies in addition to LV GLS and/or LV MD. Thirdly, although a similar score criterion was available (changes in LV GLS and LV MD values per 1% and 10 ms, respectively), that allowed them to be combined in a meta-analysis depending on the endpoint of the study. It should be remembered that the quality of the echocardiographic imaging and the appropriate imaging settings are crucial to assess myocardial strain (e.g., frame rate between 50 and 70 fps). In addition, it should be noted that in the studies, the assessment of echocardiographic parameters was carried out with various devices and software used for data post-processing, as well as by various operators.
Conclusion
LV GLS and LV MD assessed using speckle tracking provides important predictive value in patients with ischemic and nonischemic cardiomyopathy. Prospective multicenter studies with a large patient population and longer follow-up period are needed to validate the results and assess the feasibility of implementation in clinical decision-making.
Relationships and Activities: none.

Чтобы читать статью войдите с логином и паролем от scardio.ru
Keywords
For citation
Golukhova E.Z., Berdibekov B.S., Ruzina E.V. Efficacy and safety of combined aspirin and warfarin therapy after heart valve replacement: a systematic review and meta-analysis of randomized clinical trials. Russian Journal of Cardiology. 2022;27(3S):4933. https://doi.org/10.15829/1560-4071-2022-4933
Copy